Patient Policies
NOTICE OF PRIVACY PRACTICES
This notice describes how health information about you may be used and disclosed and how you can get access to this information. Please review it carefully. The privacy of your health information is important to us.
OUR LEGAL DUTY
We are required by applicable federal and state law to maintain the privacy of your health information, we are also required to give you this notice about our privacy practices, our legal duties, and your rights concerning your health information. We must follow the privacy practices that are described in this notice while it is in effect. This notice takes effect 10/17/2002, and will remain in effect until we replace it.
We reserve the right to change our privacy practices and the terms of this notice at any time provided such changes are permitted by applicable law. We reserve the right to make the changes in our privacy practices, we will change this notice and make the new notice available upon request. You may request a copy of our notice at any time. For more information about privacy practices or for additional copies of this notice, please contact us using the information listed within.
USES AND DISCLOSURES OF HEALTH INFORMATION
We use and disclose health information about you for treatment, payment, and healthcare operations. For example:
Treatment: We may use or disclose your health information to a physician or other healthcare provider providing treatment to you, when coordination of care is applicable.
Payment: We may use and disclose your health information to obtain payment for services we provide you.
Healthcare Operations: We may use and disclose your health information in connection with our healthcare operations. Healthcare operations include quality assessment and improvement activities, reviewing the competence and qualifications of healthcare professionals, evaluation practitioner and provider performance conducting training programs, accreditation, certification, licensing or credentialing activities.
Your Authorizations: In addition to our use of your healthcare information for treatment, payment or healthcare operations you may give us written authorization to use your health information or to disclose it to anyone for any purpose. If you give us an authorization, you may revoke it in writing at any time. Your revocation will not affect any use or disclosures permitted by your authorization while it was in effect. Unless you give us a written authorization we cannot use or disclose your health information for any reason except those described in this notice.
To Your Family and Friends: We must disclose your health information to you as described in the Patient Rights section of this notice. We may disclose your health information to a family member, friend or other person to the extent necessary to help with your healthcare or with payment for your healthcare but ONLY if you sign an informed consent to disclose such information naming the specific party to be included in the use and
disclosure of your information.
Marketing Health-Related Services: We will not use your health information for marketing communications without your written authorization.
Required by Law: We may use or disclose your health information when we are required to do so by law.
Abuse or Neglect: We may disclose your health information to appropriate authorities if we reasonably believe you are a possible victim of abuse, neglect, or domestic violence or the possible victim of other crimes. We may disclose your health information to the extent necessary to avert a serious threat to your health or safety or the health and safety of others.
National Security: We may disclose to military authorities the health information of Armed Forces personnel under certain circumstances. We may disclose to authorized federal officials health information required for/or pertinent to issues of national security. We may disclose to correctional instituion or law enforcement officials having lawful custody of protected health information of inmate or patient under certain circumstances, as with court-ordered writ.
Appointment Reminders: We may use or disclose our health information to provide you with appointment reminders, such as; voicemail, postcards, or letters.
PATIENT RIGHTS
Access: You have the right to look at or get copies of your health information with limited exceptions. You have the right to request a written record of any disclosures of health information that may have taken place during treatment, payment or healthcare operations. You may request that we provide copies in a format other than photocopies. We will use the format you request unless we cannot practically do so. You must make a request in writing to obtain access to your health information. You may obtain a form to request access by using the contact information listed on this notice. We may charge you a reasonable cost-based fee for expenses such as copies and staff time, please contact regarding fee structure.)
Restriction: You have the right to request additional restrictions on your health information. We are not required to agree to these additional restrictions, but we will accommodate your privacy within reasonable limits and to the extent of our power.
Amendment: You have the right to request we amend your health information. Your request must be in writing and must explain why the information should be amended. We may deny your request under certain circumstances.
QUESTIONS AND COMPLAINTS
If you want more information about our privacy practices, or have questions or concerns, please contact us. If you are concerned about your privacy rights or disagree with the use or disclosure of your private health information, you may contact us directly. You may also submit a written complaint to the U.S. Department of Health and Human Services. We support your right to the privacy of your health information.
Office of Jerry C. Hu, DDS
Phone: 907.262.6466 Fax: 907.260.3459
125 North Binkley St., Soldotna, AK 99669
12570 Old Seward Hwy. Ste. 201, Anchorage, AK 99515
To view our Notice of Privacy Practices in PDF format, please click here.
OUR LEGAL DUTY
We are required by applicable federal and state law to maintain the privacy of your health information, we are also required to give you this notice about our privacy practices, our legal duties, and your rights concerning your health information. We must follow the privacy practices that are described in this notice while it is in effect. This notice takes effect 10/17/2002, and will remain in effect until we replace it.
We reserve the right to change our privacy practices and the terms of this notice at any time provided such changes are permitted by applicable law. We reserve the right to make the changes in our privacy practices, we will change this notice and make the new notice available upon request. You may request a copy of our notice at any time. For more information about privacy practices or for additional copies of this notice, please contact us using the information listed within.
USES AND DISCLOSURES OF HEALTH INFORMATION
We use and disclose health information about you for treatment, payment, and healthcare operations. For example:
Treatment: We may use or disclose your health information to a physician or other healthcare provider providing treatment to you, when coordination of care is applicable.
Payment: We may use and disclose your health information to obtain payment for services we provide you.
Healthcare Operations: We may use and disclose your health information in connection with our healthcare operations. Healthcare operations include quality assessment and improvement activities, reviewing the competence and qualifications of healthcare professionals, evaluation practitioner and provider performance conducting training programs, accreditation, certification, licensing or credentialing activities.
Your Authorizations: In addition to our use of your healthcare information for treatment, payment or healthcare operations you may give us written authorization to use your health information or to disclose it to anyone for any purpose. If you give us an authorization, you may revoke it in writing at any time. Your revocation will not affect any use or disclosures permitted by your authorization while it was in effect. Unless you give us a written authorization we cannot use or disclose your health information for any reason except those described in this notice.
To Your Family and Friends: We must disclose your health information to you as described in the Patient Rights section of this notice. We may disclose your health information to a family member, friend or other person to the extent necessary to help with your healthcare or with payment for your healthcare but ONLY if you sign an informed consent to disclose such information naming the specific party to be included in the use and
disclosure of your information.
Marketing Health-Related Services: We will not use your health information for marketing communications without your written authorization.
Required by Law: We may use or disclose your health information when we are required to do so by law.
Abuse or Neglect: We may disclose your health information to appropriate authorities if we reasonably believe you are a possible victim of abuse, neglect, or domestic violence or the possible victim of other crimes. We may disclose your health information to the extent necessary to avert a serious threat to your health or safety or the health and safety of others.
National Security: We may disclose to military authorities the health information of Armed Forces personnel under certain circumstances. We may disclose to authorized federal officials health information required for/or pertinent to issues of national security. We may disclose to correctional instituion or law enforcement officials having lawful custody of protected health information of inmate or patient under certain circumstances, as with court-ordered writ.
Appointment Reminders: We may use or disclose our health information to provide you with appointment reminders, such as; voicemail, postcards, or letters.
PATIENT RIGHTS
Access: You have the right to look at or get copies of your health information with limited exceptions. You have the right to request a written record of any disclosures of health information that may have taken place during treatment, payment or healthcare operations. You may request that we provide copies in a format other than photocopies. We will use the format you request unless we cannot practically do so. You must make a request in writing to obtain access to your health information. You may obtain a form to request access by using the contact information listed on this notice. We may charge you a reasonable cost-based fee for expenses such as copies and staff time, please contact regarding fee structure.)
Restriction: You have the right to request additional restrictions on your health information. We are not required to agree to these additional restrictions, but we will accommodate your privacy within reasonable limits and to the extent of our power.
Amendment: You have the right to request we amend your health information. Your request must be in writing and must explain why the information should be amended. We may deny your request under certain circumstances.
QUESTIONS AND COMPLAINTS
If you want more information about our privacy practices, or have questions or concerns, please contact us. If you are concerned about your privacy rights or disagree with the use or disclosure of your private health information, you may contact us directly. You may also submit a written complaint to the U.S. Department of Health and Human Services. We support your right to the privacy of your health information.
Office of Jerry C. Hu, DDS
Phone: 907.262.6466 Fax: 907.260.3459
125 North Binkley St., Soldotna, AK 99669
12570 Old Seward Hwy. Ste. 201, Anchorage, AK 99515
To view our Notice of Privacy Practices in PDF format, please click here.
DISCRIMINATION
The offices of Dr. Jerry C. Hu, DDS, Family Dentistry, LLC comply with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex.
Dr. Jerry C. Hu, DDS, Family Dentistry, LLC does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
Dr. Jerry C. Hu, DDS, Family Dentistry, LLC:
Provides free aids and services to people with disabilities to communicate effectively with us, such as:
If you need these services, contact our Office Manager. If you believe that Dr. Jerry C. Hu, DDS, Family Dentistry, LLC has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with:
Dr. Jerry C. Hu, DDS, Family Dentistry, LLC
c/o Office Manager
125 N. Binkley St.
Soldotna, AK 99669
(907) 262-6466
(907) 260-3459 - Fax
office@smilesofalaska.com
You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, Office Manager is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services
200 Independence Avenue SW.
Room 509F, HHH Building
Washington, DC 20201
Toll Free: 1-800-868-1019,
800-537-7697 (TDD).
Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
Dr. Jerry C. Hu, DDS, Family Dentistry, LLC does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
Dr. Jerry C. Hu, DDS, Family Dentistry, LLC:
Provides free aids and services to people with disabilities to communicate effectively with us, such as:
- Qualified sign language interpreters
- Written information in other formats (large print, audio, accessible electronic formats)
- Qualified interpreters
- Information written in other languages
If you need these services, contact our Office Manager. If you believe that Dr. Jerry C. Hu, DDS, Family Dentistry, LLC has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with:
Dr. Jerry C. Hu, DDS, Family Dentistry, LLC
c/o Office Manager
125 N. Binkley St.
Soldotna, AK 99669
(907) 262-6466
(907) 260-3459 - Fax
office@smilesofalaska.com
You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, Office Manager is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services
200 Independence Avenue SW.
Room 509F, HHH Building
Washington, DC 20201
Toll Free: 1-800-868-1019,
800-537-7697 (TDD).
Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
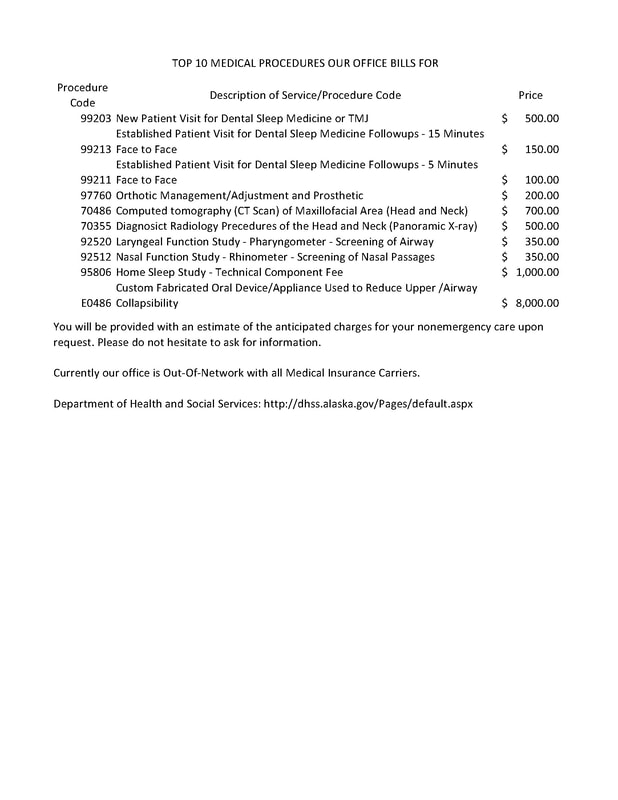
TOP 10 MEDICAL PROCEDURES WE BILL